
Is it time to acknowledge that mistakes were made during the period referred to as the Covid-pandemic?

We recently contemplated the impact of our new manuscript on policy lessons learned during the Covid-19 period, which was published in the International Journal of Public Health “What Lessons Can Be Learned From the Management of the Covid-19 Pandemic?”
Together with our 36 co-authors (including MDs, economists, sociologists, statisticians, research scientists and other professionals) we tried to summarize what we thought were the key policy mistakes during the period referred to as the ‘Covid-pandemic’ and then offer solutions for future scenarios.
We realize that there are many scientific opinions on the whole management of Covid-19 at that period, and that we do not speak for all scientists. Neither do we agree exactly among ourselvs on all the facets of these decisions, but, we do agree on the issues we have highlighted in this manuscript. In addition, we realise there are deep divisions in science over this period which we have covered extensively in a previous manuscript-
A Tale Of Two Scientific Paradigms: Conflicting Scientific Opinions On What Following The Science Means For SARS-CoV-2 and the Covid-19 Pandemic, https://www.researchgate.net/publication/353837019.
Although we anticipated that there would be those who did not agree with our analysis and would push back as soon as it was published, it turned out that there was very little debate and after a brief flurry on twitter and a few podcasts, our analysis seems to have sunk to the bottom of the media ocean, although we did briefly notice that we were big in Japan! Thanks for the retweet Dr Hideki Kakeya, Dr.Eng. @hkakeya
Although many people don’t want memories of this period dredged up, we cannot have complete closure on this subject or move on unless a full acknowledgment of mistakes is made. Future health policies cannot be built on top of substandard foundations.
For those that say that, yes it was an emergency and mistakes were bound to be made, we offer extensive evidence that policy makers knew many policies had no real scientific validity and yet were often repeated! Or that certain medications that caused adverse events are still being recommended. Does an "emergency" really mean that we should scrap established scientific protocol?
We realize that even though we wrote our peer-reviewed article in what we thought was our simplest scientific language, its message was still not easily understandable to a general audience. Therefore, this Substack is an attempt to retranslate its main messages.
2. Why we specifically chose peer review.
Historically, many of the co-authors on our manuscript had already come to independent assessment that there was something oddly amiss about the Government and health authorities’ response to what the WHO referred to as ‘the Covid-19 pandemic’. We say ‘referred to as a pandemic’ here because many of us thought that this was a stretch of the previous definition of a pandemic but seemingly in this day and age many term seem to have a built-in official flexibility. Still, the authors used ‘official’ terminology throughout the manuscript because it was familiar during this period.
It was only after a period of time had passed that it dawned on most co-authors that their objections to Covid policies were being deflected or falling on deaf ears ! This was especially worrisome since the general public were only being informed about one side of the scientific debate and relied on this information to make informed decisions on their health.
Many of our co-authors felt very strongly that health data and advice emanating from official sources during the Covid period was being heavily manipulated to lean into an official ‘science’ narrative and (maybe for political reasons) that no other interpretations were to be tolerated. However, it is harder to maintain a fiction than simply to tell the truth, especially in emerging research. That is why a lot of the official pronouncements didn’t ring true to our panel of authors. Many of the co- authors were already trying to make their objections to official Covid-19 health policies heard. Some belonged to different advocacy groups such as the Health Advisory and Recovery Team (HART) or had already signed the Great Barrington Declaration (GBD) which had laid out alternatives to government suggestions. But even this strength of numbers was not enough to be heard in mainstream media or other media channels for that matter. Indeed, although they were widely supported, the three authors of GBD declaration faced routine hit pieces and were smeared as ‘fringe epidemiologists’ in some media. Other advocacy groups such as HART were similarly vilified and even had their personal communications hacked by ‘concerned citizens‘ and disseminated into smear pieces in the media.
The other co-authors in our current manuscript have also had their personal battles with media smears, manuscript retractions and institutional pressures. In some cases scientific journals would even retract manuscripts after they had passed peer review and been published just because of external pressures. Many of the excuses for this behaviour were scientifically absurd as co-authors Harald Walach, Beny Spira, Norman Fenton and Jessica Rose found out.
Of course the other route for the dissemination of scientific ideas is to publish scientific material as a pre-print, which usually occurs just before the peer review process. However, when it came to the topic of Covid, even pre-print servers were nervous and reluctant to publish. Even if articles were eventually published in pre-print, they were often dismissed as not being properly scrutinized science.
Of course like this translation of our article, some people already publish their thoughts in a Substack ! While this is very useful in discussing events, it is not subject to feedback or challenges from suitably qualified professionals, however, the subject of Covid policies already has quite a complexity of subject matter so there are very few reviewers that could be considered experts.
This takes us to the peer review process itself. All the authors of this manuscript were already aware that discussion of Covid policies was very controversial and that there was almost certainly an unofficial firewall policy operating against authors who disagree with the official narrative for most scientific journals at some level.
However, the information in our current manuscript is not new. It is the amalgamation of three previous manuscripts on Covid, plus thoughts from other authors. Our first manuscript discussed what seemed like a division in scientific opinion in relation to Covid policies and we tried to explain the use of models in health policy decisions. This manuscript called “A Tale Of Two Scientific Paradigms: Conflicting Scientific Opinions On What Following The Science Means For SARS-CoV-2 and the Covid-19 Pandemic, https://www.researchgate.net/publication/353837019 only progressed as far as a pre-print and was then rejected. Additionally, on this topic some of my colleagues think that there wasn’t really a ‘division in science’. Instead, there was those advocating scientific options and those who were promoting political science ideology masqueraded as science.
Our second manuscript asked the rather innocuous question: "Did government policies or even vaccines have any effect on the rises and falls of official recorded deaths and cases?" We concluded in this manuscript that most of the influence on the pandemic came from the seasons. This simple discussion paper took two years to be published, passing through 5 journals and 12-14 reviewers on the way.
“Influence of Seasonality and Public-Health Interventions on the Covid-19 Pandemic in Northern Europe. Journal of Clinical Medicine.” https://doi.org/10.3390/jcm13020334
Our third manuscript covered government policies known as non-pharmaceutical interventions. Maybe using the word “unintended” in the title finally helped to push this one through peer review, although this topic is highly contested since policy makers used nudge units to increase fear and anxiety which have negative effects on the immune system.
“Unintended Consequences of Covid-19 Non-Pharmaceutical Interventions (NPIs) for Population Health and Health Inequalities.” https://doi.org/10.3390/jcm13020334
This brings us to our current manuscript which highlights mistakes in the government’s approach to Covid. It has been more than 2 years in the making and has been submitted to several scientific journals. We are grateful to the International Journal of Public health, which is more than 100 years old, for now having the courage to publish our work!
However, as we have stated, although the manuscript might have been understood by certain professionals within the public health field, this is not our main goal.
This being said, there are probably very few people left on the planet that are untouched by the consequences of either Covid or Covid policies. Therefore, our manuscript and analysis is also intended for these people. Unfortunately, the language and level of proof of peer reviewed journals is very exact and does not lend itself to easy understanding by people outside this field. This is why we are taking the time to spell its meaning.
3. Let’s start at the very beginning!
The introduction to our manuscript starts by making the best possible argument for the official government position on Covid-19 policies. In some circles this form of debate is known as a “steel man’’. This is the opposite of a straw-man where people try to make a very weak case for their opponent so that they can demolish is easily. In this way we feel we cannot be accused of having a kangaroo court review of the subject. After this introduction, we present the (mostly) official data from the pandemic over a period of three years. We try not force our opinion in this section but rather we (try to) allow the reader to make up their own mind as to whether the government health policies were mistaken or not. As some people describe it, “we supply the raw ingredients and the reader bakes the cake”.
We think this approach works very well in the peer review format, allowing for some disagreements with reviewers along the way. However, some readers have already misinterpreted our attempts to be fair as not sufficiently condemning the government approach. Although all the authors of our manuscript had very strong opinions, strong pejoratives are not the language of balanced scientific articles, rather we rely on the data presented to give people sufficient knowledge to make up their own mind.
4. The human cost of disease and government responses
We are well aware that the collective voices of all of our authors are not just some academic disagreements on the relative merits of scientific policies but rather about real lives lost, and the economic and social fallout of government policies.
Although most governments described their approaches as scientific, some of my colleagues would say that they were not derived from the ‘scientific method’ but rather they were political decision presented in what looked like a scientific manner to the large percentage of the population who are not particularly trained in this subject!
To be clear, what the authors of this study do not say is that there no such thing as a SARS-CoV2 virus, although we understand from the original paper on the PCR test which was used to confirm Covid, that it used a wide mix of genetic sequences derived from known sequences both of bat viruses and viruses isolated from humans that might have been responsible for SARS-like symptoms.
(Corman, Drosten et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. https://pmc.ncbi.nlm.nih.gov/articles/PMC6988269/).
Many of us also think that there was a contagious respiratory illness that was prevalent at the initial time of Covid. On my part (GQ) I remember contracting some respiratory disease at this time characterized by sudden tiredness and distressing respiratory problems for several days. My respiratory problems lingered like some sort of post-viral syndrome for several years afterwards! Indeed, several of our co-author colleagues reported similar events concerning respiratory infections.
5. The skewed presentation of data, facts and figures.

Figure 1. Mountains out of molehills!
Many of us have different recollections of the beginnings of the Covid pandemic. Many of us heard vague reports from the Wuhan institute accompanied by video footage of sudden deaths in the street. This was followed by some very dramatic reporting from the Italian resort of Bergamo and finally culminated in the WHO declaration of a pandemic.
Despite this barrage of media reports, the main foundation of the (UK) government policies came from mathematical models of a potentially overwhelming epidemic. These are discussed extensively in the first part of the manuscript. However, as we state, although models are sometimes useful, the Covid models were useless and were rather used as a coercive tool for government policies.
Some colleagues have noted that we are increasingly told to listen to experts, adhere to consensus, follow computer projections, etc. They say this is now being taught in US K-12 schools and is absolutely intended to discourage citizens from thinking on their own (critical thinking).
That said, the reality is that most computer projections of complex matters are shockingly inaccurate. No model should be accepted unless ALL assumptions are spelled out in detail, including the values of EVERY variable, and the projected relationships between variables. Unfortunately for most people the models were a ‘black box’ so in the manuscript we attempted to explain their use during the Covid period.
Essentially the models were based on the mathematical equation for the progression of a pandemic that follows a symmetrical bell shaped curve. This was devised about 100 years ago by two biochemists after the 1918 pandemic. This model (SIR) assumes that everybody is susceptible to a disease (S), everybody then becomes infected as time progresses (I) and then most people recover (R) from the disease or die! Therefore, the model is called an SIR model. One of my colleagues has since reminded me that there is no scientific basis for a complex matter like Covid-19 following a bell curve.
This SIR model or derivatives of it are essentially still used today to model pandemics. There are very complicated versions of these models which also take into account many variables but these were not considered by policy makers or at least not used as the basis of policy decisions.
One of the main problems is that, even though the more complex models predicted the movements of some people and therefore their potential contacts and the spread of disease, they still did not properly consider the biology or immunology of the process! Considering that these models were developed in 1927, that’s a lot of biology missing!
In order to predict anything with these SIR models, the input assumptions must be at least nearly correct. However, in our manuscript we discuss how these models only really fit with the notion that people in populations are like identical units. Some models obviously have flexibility in considering some people will move between places with more frequency.
Lack of sufficient biological and immunological considerations led to ‘one size fits all’ policies, however, most people were aware that young people and old people were not susceptible to the same risks of infection (as discussed in GBD). In fact, the immunity of young people seemed to rely on more innate immune mechanisms than the acquired immune system, i.e. antibodies etc. Additionally, the models did not consider that some people might have some prior immunity from prior exposure to similar cold viruses. As can be seen from Figure 2, the immune system is very complex!

Figure 2. A schematic comparison of the main features of innate immunity (left) and acquired immunity (right) and how they might interact with SARS-CoV-2. Pathogen pattern recognition receptors (PRR) Thymus derived cells (T-Cells) B-lymphocytes (B-cells).
{Some of my colleagues have noted that throughout the whole Covid-19 matter, key aspects of the immune system were curiously ignored. Many clinicians involved in decision making during this time barely mentioned this topic, and if they did it was only to emphasise that the new medicines were superior to natural immunity.}
It also seemed obvious in the pre-Covid period that many respiratory diseases tended to have seasonal peaks i.e. high in winter and low in summers. However, Covid models began at day 1 and made no allowance for seasonality. So, when certain government interventions were applied and the numbers of cases and deaths seemed to fall, the policy makers claimed that their strategies were working, rather than it being because of the usual seasonal decline after cold and flu season. This was pointed out by Simon Wood, however his manuscript on this topic was unaccountably delayed for more than a year so that the general public never got to hear about his work in time to have an informed opinion.
Actually, we think that it’s quite obvious that sub-optimal inputs were the reason that the models failed to predict anything close to the actual data. Or as some people say, garbage in – garbage out. For instance, the morbidity predictions in Sweden were off by a factor of six-fold and similarly, UK predictions were sometimes off by a factor of 20-fold.
Of course, these exaggerated scenarios were not made any more realistic by the ever changing definitions of Covid deaths and causes. At the beginning of the pandemic in the UK, data on positive cases was linked to the NHS central register of patients who died. This meant that a patient who tested positive would be counted as a Covid death even if they died months later from another cause. This definition was later changed to report deaths within 28 days of a first positive laboratory-confirmed test.
Perhaps a simpler example is that when a motorcyclist died in a motorcycle accident, it was counted as a Covid death if they tested positive for Covid.
Another factor in the inflation of case and death numbers was the PCR test developed by Drosten. The threshold for detection of virus in the PCR test (developed by Drosten) was set very high, indeed in some cases, more than 40 cycles of PCR. Bear in mind that each cycle of PCR doubles the amount of DNA in the reaction. Although official authorities said that the high cycle thresholds were an attempt to also detect pre-symptomatic cases, this high sensitivity would also detect disintegrating fragments of virus. Indeed a paper by Dr. Rita Jaafar showed that virus cultivation (from specimens) was rare above 35 PCR cycles and that these rare cases should not impact public health decisions.

Figure 3. Relationship between the cycle threshold (Ct) required before testing positive in a Covid-19 PCR test and the probability that the virus can be cultured in the laboratory from the swab. Results are taken from published data from the La Scola lab in Marseille, France and are adapted from Figure 1 of Jaffar et al. (2020). (a) Jaffar et al. attempted to culture the virus from 3790 samples which had tested positive in a RT-PCR test for the “E” gene of SARS-CoV-2, and sorted their results according to what cycle threshold (Ct) was required before testing positive. (b) 1941 (51%) of the samples could be cultured in the laboratory, but the % declined rapidly with increasing Ct.
6. Official measures to protect the people: Government interventions
The scenarios suggested by the official models of Covid and their projected impacts, were also used as the justification for many of the government policies. Many of these policies might have had some theoretical rationale but they were never been field tested. Those that were field tested pre-Covid were found to be inadequate in several reports. As an illustration as to how ‘seriously’ the UK government were taking the situation, one of the ministers commented that the pandemic was also an opportunity for some of his colleagues to introduce pet-projects that they always wanted to try.
Of course, many governments already had pandemic preparedness plans in place for the outbreak of a respiratory disease. But as previously mentioned, these were discarded in favour of a new set of experimental ideas.
Although there are now attempts to rewrite the history of this period and say that rules made during the Covid period were only advisory, some rules were strictly enforced such as masking, gathering, and staying at home. Sometimes even law enforcement wasn’t that sure of the legal backing for these policies. Who could forget the sight of police chasing joggers along the beach because of this emergency? Even supermarket security staff were used as unofficial enforcers of some mask-wearing policies, delving into people’s medical history without any training in medical confidentiality to find out why they had an exemption.
The inconsistencies were clear to even laypeople. For example it was fine to intermix with hundreds of others at Walmart, but they were prohibited from being in a Church pew.
We have written extensively on the policy of masks in several of our manuscripts. Needless to say, if there was strong scientific evidence to prove that they were effective in reducing the spread of airborne viruses in the community, then it would be trumpeted as definitive proof. As it was, there were a number of studies with very weak evidence, that even when bundled together were not very convincing. There were also randomized control studies, the gold standard of clinical proof, such as the Bangladesh study which was neither properly controlled nor randomized. In fact, the study was so full of inconsistencies that many papers were written about its mistakes.
One can only conclude that policies such as mask wearing were more about appearing to do something, as well as forcing conformity and obedience, rather than anything to do with public health.
Of course, we also talk about the other side of government interventions which are the physical, social and economic harms. There are other studies that look into the subject of safety https://c19science.info/Covid-19_Masks.pdf
To list these shortly, immunity was threatened by long periods behind masks, being locked down or even having a negative outlook upon events. Rules created divisions in society which were exacerbated by digital and physical separation measures such as digital passports! There was even an increase in suicides. As one of my colleagues put it
“the side effects of the (Covid) measures hit like a tsunami: stress, obesity, drug addiction, mental illness, collapsed healthcare systems, economic ruin, disrupted education, and lonely deaths among the elderly. The ultimate irony? Policies meant to protect people from Covid fuelled obesity, which turned out to be one of the biggest risk factors for severe Covid outcomes. It was a classic medical error—where the cure is more dangerous than the disease—executed on a societal scale.”
Although many professionals tried to highlight lifestyle and dietary changes that could alleviate some of the symptoms of the disease, reduce its severity and perhaps boost immunity, these were not widely promoted by health authorities.
7. Balanced pharmaceutical evaluation.
It may not have been obvious to everybody during the Covid period that there were some relatively safe repurposed drugs that were initially proposed as a treatment for Covid. Other physicians also offered a list of diet and lifestyle adjustments which might offset the damage from Covid or to help in prevention! Even simple supplements such as Vitamin D (which had numerous scientific studies concluding that it was effective) were ignored. However, in our manuscript we mainly concentrate on the seemingly unequal assessment of the safety and efficacy of repurposed clinical drugs versus the new genetic vaccines. There were many in the medical community who advocated repurposed drugs like ivermectin (IVM) and hydroxychloroquine (HCQ) for the treatment of Covid when the official position was to do nothing. The prescription of these repurposed drugs was rapidly shut down by official sources and in some instances the mention of these drugs was banned from social media as disinformation.
However, in the manuscript we make the point that even if repurposed drugs were only 40% or 60% effective in treating Covid (which some of them were even by official statistics BMJ/WHO report) and also had a long safety track record, like ivermectin and hydroxychloroquine, wouldn’t this be preferable to doing nothing? If it was a real emergency, why would the health authorities want to wait nine months before they provided an official sanctioned product that would reduce Covid-19? In their report, A living WHO guideline on drugs for Covid-19 published on the BMJ website they state that both hydroxychloroquine (HCQ) and ivermectin (IVM) were not to be used under any circumstances.
A living WHO guideline on drugs for Covid-19 https://www.bmj.com/content/370/bmj.m3379
Some of our USA colleagues informed us that (in their opinion) the entire EUA process (FDA) was completely compromised when it came to the assessment of repurposed drugs. Further, it was not designed to give patients accurate information so that they can make a health choice that is in their best interest.
8. Do we really have to discuss the new genetic vaccine technology?
The quick answer to this is yes! We were particularly curious as to why did health authorities and drug companies pick the time of a pandemic to introduce a novel technology? Bearing in mind that releasing any pharmaceutical product always carries an element of risk! Was it because there was a captive audience with no official alternative treatments? Was it because this technology was not consistent enough to pass a normal assessment and needed Emergency Use Authorization (EUA) to get it across the line? Would people have rushed to take the ‘vaccine’ if it were described as a gene therapy or even a genetic technology?
The fact is, as we have discussed in our manuscript, that this technology is different from the regular or traditional method of vaccine manufacture. We think that many people were fooled into believing that the new genetic vaccines were similar to traditionally manufactured vaccines and therefore would have a similar safety record. But these were definitely not the same thing!
For proof of that, early on in Covid, the CDC changed their longtime official definition of what a vaccine is, to accommodate the experimental mRNA Covid injection.
In brief, the genetic material in the vaccine is injected into the body encapsulated in lipid nanoparticles or enclosed in a viral vector and carries instructions to the cells of your body to start making (active) parts of an organism that causes disease. It is uncertain how many different types of cells these genes will enter, but the immune system will target all these cells and theoretically destroy them. These could be heart cells, brain and nerve cells, circulatory cells etc.
There were all sorts of wild ideas appended to this technology. We think this might have been over-exuberance on the part of the tech people because immunologists or biologists would never think of these things.
The first promotion was the 100 day vaccine idea, from design to clinical use. It logically sounds better to have a rapid process, almost like science fiction but that’s just what it was, just fiction without knowledge of biological or immunological reality and the potential harms that can be caused by mis-steps. It is painful to see that physiological and immunological understandings gleaned from years of painful and sometimes tragic mistakes could be discarded because some tech or business people want to cut the red tape and go faster. We are not aware of any human system that runs on 100 day cycles! New drugs take time to develop and test because time is also a factor in identifying potential safety signals. In this situation zero long term safety tests were done of the Covid injections.
Another hare-brained notion that some people were trying to push across the line, was the ‘plug and play’ system. This involves the design of an original template product, which is the DNA/RNA code for the (virus) protein and then adjusting each new version to suit a new variant. This also sounds logically plausible but immunologically and physiologically disastrous or at the very least like Russian roulette!
The plug and play answer was used in response to the waning of vaccine efficiencies and the emergence of resistant variants but this idea really breaks too many ethical and testing rules. Each new protein or chemical has to be tested on its own and not assumed to have a similar safety profile as older drugs. Although memories seem to be very short for people proposing this idea or maybe they were not born yet, but in the 60s we had the tragedy of thalidomide.
Thalidomide can be found in a D (+) and L (-) form, which are optical isomers. The difference between the two forms is that the L form will cause teratogenic mutations to the offspring of pregnant woman and the D form is a sedative. Testing agencies were always very well aware that seemingly small changes in drugs can make great differences in drug pharmacokinetics !!!!
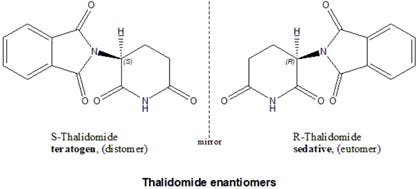
Figure 4. Comparison of Thalidomide enantiomers (non-superimposable mirror images).
This brings us to the discussion of the safety and efficacy of the new genetic vaccines as tested in the vaccine trials. In drug trials, efficacy means how well a drug performs in ideal, controlled circumstances to produce a desired therapeutic effect. In the vaccine trials efficacy is presented in terms of risk reduction. i.e. how much this vaccine will reduce the chances of catching symptomatic Covid compared to a normal situation.
Table 1. Drug trials of Covid vaccines with the number of participants, cases of officially conformed symptomatic Covid and the number of trial sites. Relative risk reduction (RRR), absolute risk reduction (ARR).

While rates of 66%–95% relative risk reduction look impressive, only 0.5%–1.2% of the trial participants in either the vaccine or control arms (no vaccine) were identified as confirmed cases during the genetic vaccine trials. In comparison, the absolute risk reduction (ARR) numbers were miniscule, barely 1%. To present one measurement RRR without the other ARR is incredibly misleading. How many citizens would line up for an experimental Covid injection if they knew that the absolute risk reduction was about 1%?
One of the reasons why only 0.5%–1.2% of trial participants in either arm of the vaccine trials were identified as symptomatic Covid cases during the trials is that many participants with suspected but unconfirmed Covid-19 were not included in the RRR calculations. For example, for the Pfizer trials, while the RRR of 95% was based on 170 confirmed cases (of which 95% were in the placebo group), there also were “1594 cases of suspected but unconfirmed Covid-19 in the vaccine group vs. 1816 in the placebo group”. Hence, the number of participants with “suspected but unconfirmed Covid-19” was 20 times higher (3,410) than the 170 confirmed cases used for calculating RRR. Additionally, a further 371 participants (311 from vaccine group vs. 60 from placebo group) were excluded from efficacy analysis for “important protocol deviations on or prior to 7 days after Dose 2”. It is still unclear how many of the 3,410 suspected but unconfirmed cases in the Pfizer trial would have been confirmed cases if adequately tested and how this would have affected the RRR.
Trial site inspection staff later came forward to reveal that personnel at some trial sites knew who was given the vaccine and who was given the placebo, potentially biasing the decisions of staff on whether to call trial participants in for Covid tests.
In addition to this, Norman Fenton also points out in this video that for the first 14 days, patients that are vaccinated are classified as unvaccinated, therefore adding to the tally. “Cheap trick vaccine efficacy Illusion for a typical observational study”
The officially available trial data was reanalysed by some researchers who found that there were 0.10%–0.15% serious adverse reactions relative to the placebo arm, i.e., “uncommon” rather than “very rare” as originally claimed.
It is also extremely concerning that some of the severe adverse reactions to the new genetic vaccines were omitted from papers describing the trial results. Some of these trial participants said they experienced psychological manipulation (“medical gaslighting”) rather than medical support from the trial organisers and they are still struggling with severe vaccine injuries for long after these trials ended.
9. From very rare to common, tracking adverse events from the new genetic type vaccines.
Once the genetic type vaccines were approved and had received emergency use authorization, we began to see that adverse events that were previously described as very rare started to be recorded in greater numbers in the categories of uncommon or even common.
For reference:
Very rare: affecting less than 1 in 10,000 people (< 0.01%)
Rare: affecting between 1 in 1,000 to 1 in 10,000 people (0.1% to 0.01%)
Uncommon: affecting between 1 in 100 to 1 in 1,000 people (1% and 0.1%)
Common: affecting between 1 in 10 people to 1 in 100 people (1% to 10%)
As these estimates of the rates of adverse reactions increase over time, the range of conditions also increased to encompass Guillain-Barré syndrome; cerebral venous sinus thrombosis; encephalomyelitis; psychiatric adverse reactions; menstrual irregularities; tinnitus; shingles and even death in some cases.
Even the statistics that support these reports increased. A study of the French population found that among 32 million vaccinated people, 3,225 developed myocarditis or pericarditis, 97% of which were vaccine-related. The second-largest Covid-19 vaccine safety study ever conducted (n=85 million people) found increased risks of heart attack (+286% after 2nd dose), stroke (+240% after 1st dose), coronary artery disease (+244% after 2nd dose) and arrhythmia (+199% after 1st dose)
There are many other promises made over the safety of the genetic vaccines before they were administered that have been proven to be wrong by real life data. Perhaps a very important claim was that the vaccine would not persist for that long in the system. However current reports show that the spike protein encoded by the viral genome can persist for 709 days according to a report from Yale University. "Immunological and Antigenic Signatures Associated with Chronic Illnesses after Covid-19 Vaccination" https://medrxiv.org/content/10.1101/2025.02.18.25322379v2.full
In another study by Patterson et al., they found that that the spike protein persisted for up to 245 days in monocytes.
"Detection of S1 spike protein in CD16+ monocytes up to 245 days in SARS-CoV-2-negative post-Covid-19 vaccine syndrome (PCVS) individuals" https://pubmed.ncbi.nlm.nih.gov/40358138/
Although not covered in great detail in the manuscript, health authorities consistently assured the public that there was no possibility that any of the genetic technology would integrate into the human genome. However, the publications from four independent sources suggests that this might not be the case.
Aldén et al: Pfizer mRNA reverse-transcribed into DNA in liver cells. https://doi.org/10.3390/cimb44030073
Kyriakopoulos et al: Potential Mechanisms for Human Genome Integration of Genetic Code from SARS-CoV-2 mRNA Vaccination https://d197for5662m48.cloudfront.net/documents/publicationstatus/89121/preprint_pdf/7a197d8835afa569325ddec4d62f61f8.pdf
InModia Lab (Germany): Spike + SV40 found in human tissue years later. https://inmodia.de/en/about-us/
von Ranke N, McCullough PA, Catanzaro JA et al. Synthetic mRNA Vaccines and Transcriptomic Dysregulation: Evidence from New-Onset Adverse Events and Cancers Post-Vaccination. https://doi.org/10.20944/preprints202507.2155.v1
Finally, all the authors of the manuscript took issue with the unethically coercive nature of vaccine mandates “We believe that these mandates breached the core ethical principles of informed consent and bodily autonomy.”
We think that the new genetic technology was neither safe nor effective. In addition, the trials made no allowance for subjects with one or more chronic diseases who constituted a large proportion of people who contracted the disease. Finally, appropriate informed consent was not possible, as the full details of the trials, the adverse events and the nature of the new technology were not fully explained.
10. Fighting the good fight for health, WHO makes the rules?
In the final part of our manuscript, we discuss the role of governments, health agencies, the press, and non-traditional media in the creation and maintenance of a scientifically flawed narrative.
We argue that, by only considering a single set of narratives, the medical and scientific communities, as well as policymakers, were severely hindered in their ability to critically evaluate the science throughout the pandemic.
We suggest that this narrowing of the range of relevant scientific questions that were tolerated—by (a) the public (b) the media (c) social media platforms (d) the “fact-checking organisations” (e) government officials (f) the pharmaceutical industry and (g) the scientific community itself,—has inadvertently hindered the ability of researchers to engage in open-minded scientific inquiry into these complex scientific problems.
In June 2023, Facebook’s CEO made a striking confession: "Much of the content we were asked to remove turned out, in hindsight, to be accurate." In other words, most of what was deleted as "misinformation" was actually correct. Apparently, "countering misinformation" meant suppressing accurate information.
Fact-checking organizations were funded by Google and Facebook. It is hard to label information as "factual" when it contradicts the sponsor’s agenda. They labelled articles as "false," "misleading," or "lacking context" based on flimsy evidence.
Similarly in the academic world, paper retractions, which typically take two and a half years of careful scrutiny, were fast-tracked while weaker papers, seemingly on narrative, received much less scrutiny.
11. Conclusion and Recommendations
At the end of the manuscript, we make conclusions and recommendations which we have summarized into points!
1: Although mathematical and computer models can be very powerful tools, their output is directly related to input assumptions and how the programmer chooses to inter-relate variables. The models used during Covid were highly influential on public-health policies, but they bore no relation to the progression of the pandemic.
Therefore, the authors suggest that models should be treated with scepticism at the beginning of any crisis, should not be used as substitutes for analysis of the actual data and should be continuously reassessed against real data.
2. Government interventions were not effective during Covid and even had negative consequences. If any of these measures are to be considered in the future, they should be objectively assessed on the basis of real evidence and should be continuously scrutinised against real world data.
3. The discouragement of research into potential cures for Covid by repurposed medicines is scientifically and medically unacceptable. Even if some of these were partially effective at reducing Covid, further research should have been encouraged rather than discouraged.
4. Claims for the safety and efficacy of new genetic vaccines were unrealistically presented. Citizens should have been told the Absolute Risk Reduction, and that zero long term studies had been done. They did not completely prevent infection or transmission, and it is now apparent that this new therapy can cause serious adverse reactions. Although many researchers warned about just such potential risks, they were ignored or ostracized. Researchers should be able to critically evaluate claims of all new pharmaceutical products without being bullied into submission by vested interests.
5: Even though governments knew that the new genetic vaccines were not water-tight, the fact that this technology could also induce severe adverse reactions turned the vaccination programme into an unnecessary health risk. The use of mandates and coercive measures by health authorities raises considerable ethical and moral issues. Therefore, the benefit of any future drug therapies or vaccination programs should be evaluated in relevant subgroups and if necessary, dispersal should be based on genuine voluntary consent.
6: The independent nature of the consolations between doctor and patient in deciding the best healthcare pathway was compromised during pandemic especially when patients or doctors expressed an interest in repurposed drugs. Conversely, patients who expressed concern over new genetic technologies often faced considerable adversity or hostility. The possibility that this technology could be damaging was subject to medical gaslighting.
It is important that patients and physicians are allowed to work together to develop personal healthcare pathways individually designed for the circumstances of each patient.
7: Those in control of public health messages tried to supress any alternative opinions of the pandemic or government health responses. This limited access to valuable scientific information, that would allow discussion and informed choice.
We think that the best antidote to bad ideas are better ideas. Censorship of science doesn’t lead to better science just weaker conclusions. Scientific freedom should be cherished and let the truth prevail.
In answer to our first question in this Substack, is it time? The answer is definitely yes; it was time at the beginning of all of this, and it is time now. There are some who still feel they have to hold up the pillars of this crumbling edifice, but it is collapsing under the weight of its inconsistencies.
If we can have an admission of mistakes made, then the next step is accountability!
Many thanks to my co-authors for explaining some concepts to me and to John Droz for providing additional feedback.